| |
Dental enamel hypoplasia
Deficiency in enamel thickness caused by
physiological stress during the secratory
phase of amelogenesis. Hypoplasia can appear
as any form of deficiency or absence (pits,
vertical and horizontal grooves, combination
of defects) of the enamel and may be seen on
the tooth crown surface. Enamel hypoplasia
is a non-specific and sensitive indicator of
physiological stress.
 |
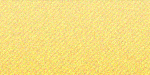
A) Ante mortem loss of the second
mandibular molar and resorption of
the alveolar bone, B) Resorption of
the alveolar bone crest revealing
the bifurcation of the first
mandibular molar root, C) Porosity
of the alveolar bone indicating
periodontal disease, D) Combination
of hypoplastic defects affecting the
mandibular canine buccal surface.
(Peqiin, Chalcolithic Period circa.
6500BP). |
|
 |
| Combination of hypoplastic
defects affecting the mandibular
canine buccal surface and linear
form of hypoplasia especially
affecting the premolars. (Peqiin,
Chalcolithic Period circa. 6500BP). |
 |
Linear form of hypoplasia affecting
the canine and arrow pointing to
calculus accumulation on the buccal
surface of the lateral mandibular
incisor. (Shiqmim, Chalcolithic
Period circa. 6500BP). |
It may occur under circumstances such as:
systematic metabolic stress (nutritional
deficiency, infection and allergy),
localized trauma or hereditary anomalies.
Since enamel does not remodel, the
occurrence of enamel hypoplasia is
indicative of physiological stress during
infancy and/or childhood at the time when
enamel was formed.
Periodontal disease
A group of diseases (gingivitis,
periodontitis, gingival abscess, periodontal
abscess) that affect the soft and hard
tissues supporting and anchoring the tooth.
The consumption of soft sticky foods
promotes the accumulation of plaque which
plays a crucial role in the progression of
periodontal disease. Accumulation of plaque
and its subsequent calcification
(infra/supra gingival calculus) may lead to
chronic or acute gingival inflammation
possibly resulting in the destruction of the
periodontal ligament at the attachment along
the root surface; the resorption of the
alveolar bone crest and finally, the loss of
the tooth prior to death.
Ante mortem tooth loss
 |
Severe ante mortem tooth loss and
alveolar bone resorption throughout
the mandibular arch (Peqiin,
Chalcolithic Period circa. 6500BP). |
The loss of the tooth prior to death as a
result of periodontal disease, pulp chamber
infection or direct trauma. The loss of the
tooth leads to the resorption of the
supporting alveolar bone.
Caries
 |
Arrows pointing to carious
lesions in the mandibular teeth. (Atlit
Yam, PPNC Period circa. 7500BP). |
A disease process involving the localized
destruction of the tooth crown. The etiology
of caries is complex and there is no
universal agreement as to its exact cause.
Nevertheless, the most widely accepted
theory is called the Acidogenic Theory in
which caries is believed to be caused by
acid producing bacteria during the enzymatic
breakdown of dietary carbohydrates. The
initial effect of the acid produced in this
process is the demineralization of the
enamel and dentine and later the destruction
of the organic portion of the affected area.
If the pulp chamber is infected an abscess
(see below) may form and the tooth may be
lost prior to death. Since dietary
carbohydrates, especially refined sugar,
play a major role in the caries process, the
prevalence of caries can be used to make
inferences regarding diet.
Dental wear
A process involving the wearing down of
the tooth surfaces by several mechanisms
which are not exclusive to each other: A)
friction of tooth on tooth , B) friction of
tooth against foreign materials, C) eroding
chemical processes other than those
involving bacteria. Wear is not defined as
pathological unless it causes pulp chamber
exposure, leading to the infection of the
pulp. Diet is a major modifying factor in
the wearing down of the tooth surface, a
tough and/or abrasive and/or chemically
erosive diet will lead to faster wear while
a refined non-abrasive, non-erosive diet
will lead to slower wear rate.
 |
A) Ante mortem loss of the second
mandibular molar, B) Occlusal wear
with cupping of the dentin. (Peqiin,
Chalcolithic Period circa. 6500BP). |
The analysis of dental wear allows
researchers to make inferences regarding
diet, food processing methods, and the
non-alimentary use of teeth. Since wear is
highly correlated with age it is used as a
tool in the assessment of individual age at
death in archaeological skeletal samples.
Nevertheless, since wear varies between
populations and even individuals, specific
wear rate calibration is needed before
making any such estimation.
Periapical abscess
An accumulation of pus in a bone cavity
around the root of the tooth, resulting from
the infection of the pulp chamber which may
be caused by a carious lesion, trauma or
severe wear. Eventually the tooth can be
lost prior to death.
 |
Abscesses in the mandibular molar
region, note the destruction of the
alveolar bone. (Peqiin, Chalcolithic
Period circa. 6500BP). |
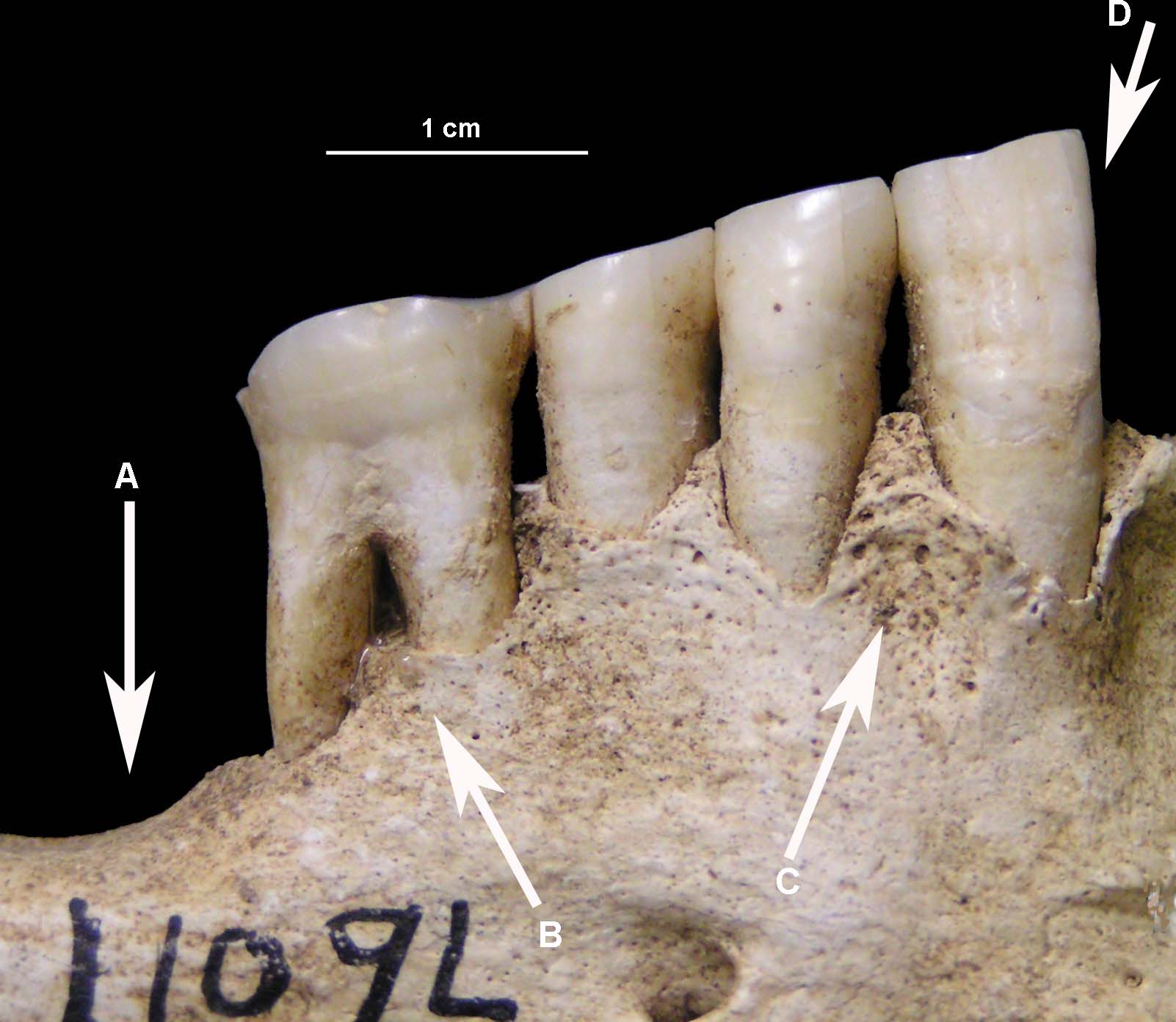
 |
Maxilla showing multiple
lesions in the alveolar bone
(C, A) and ante mortem tooth
loss (B). (Wadi Makkukh,
Chalcolithic Period circa.
6500BP). |
|
| |
 |
A) Abscess along the mesial root of
the first mandibular molar, B)
Burning. Note the severe occlusal
wear in the molar. (Wadi Makkukh,
Chalcolithic Period circa. 6500BP). |
Stages of teeth development
Initiation
The first stage is the development of the
dental lamina as a distinct narrow band in
the developing jaws. It is composed of cells
from the oral cavity ectoderm and underlying
mesenchyme. Mesenchyme and ectoderm are of
separate embryonic origin: the mesenchyme is
from the internal part of the early embryo
and is the initial tissue forming the
internal organs such as bone and muscle, the
ectoderm is from the external part and gives
rise to skin and epithelium. The process is
initiated by reciprocal signals in both
tissues. Localized swellings appear in the
dental lamina that define the location of
the future tooth bud, this swelling is the
dental placode.
Morphogenesis
Morphogenesis is the process of shape
formation. The dental placode develops into
the dental bud, in a process called budding,
which entails a fold of both ectoderm and
mesenchyme. Budding processes are also found
in the creation of other organs such as hair
follicles, mammary glands and feathers. The
bud folds once again, this time internally
and in an opposite direction to the first
fold. This marks the beginning of the cap
stage. In the topmost part of the cap the
enamel knot appears, this is a group of
cells that govern consecutive morphogenesis.
The bottom and eccentric sides of the cap
are called the cervical loop since they mark
the location of the cervical portion of the
crown. Further folding lead to the next
stage of development – the early bell stage.
In multi-cusped teeth a primary enamel knot
appears on the first cusp to develop and
secondary enamel knots appear on each of the
other cusps. In the early bell stage, each
of the cusps is folded separately at the
future occlusal portion of the tooth and the
cervical loop extends towards the cervical
portion of the tooth.
Differentiation and Mineralization
At the late bell stage the embryonic tissues
differentiate into tissues capable of
creating mineralized matrices. The ectoderm
cells differentiate into ameloblasts which
secrete a matrix that mineralizes to enamel
and the mesenchyme cells differentiate into
odontoblasts which secrete a matrix that
mineralizes to dentin. Enamel and dentin are
secreted peripherally from the junction of
the ectoderm and mesenchyme. Enamel is
secreted on top of the cusps and on the
sides of the crown. In the root of the tooth
cementum replaces enamel.
|
|